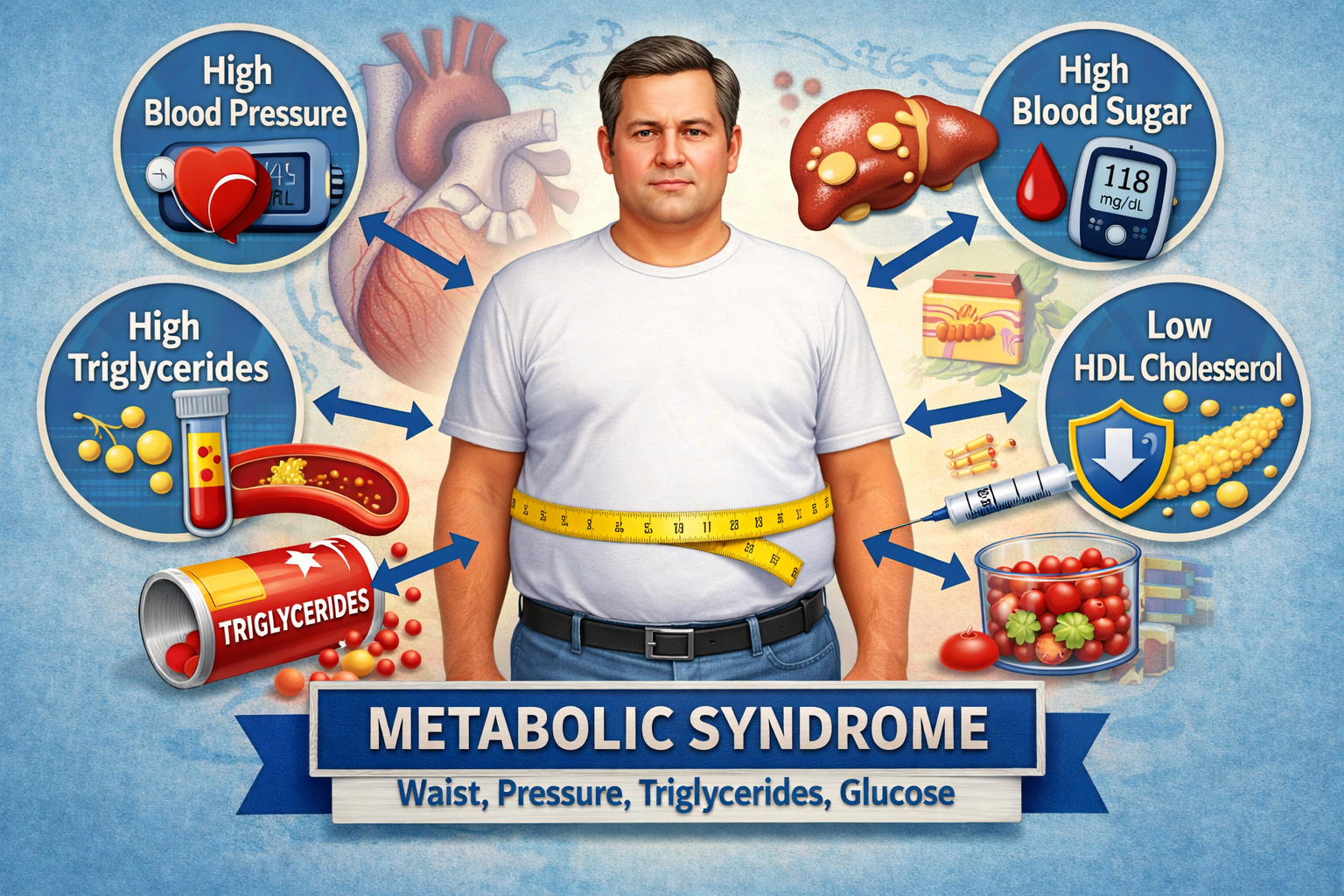


Metabolic syndrome sounds like a dense medical label, but the idea behind it is straightforward. It describes a pattern in which several metabolic problems tend to show up together: a larger waist, higher blood pressure, higher triglycerides, rising fasting glucose, and lower HDL cholesterol. Each of these markers matters on its own. When they begin clustering in the same person, the bigger story is that the body is moving into a state of chronic metabolic strain.
That is why metabolic syndrome matters far beyond endocrinology. It gives clinicians a practical way to recognize cardiometabolic risk early, before the picture becomes diabetes, stroke, coronary disease, or a full-scale cardiovascular event. It is useful because it points to a pattern, not just to one abnormal number.
What it means in plain English
In simple terms, metabolic syndrome usually reflects a body that is no longer handling excess energy efficiently, especially when fat is increasingly stored in and around the abdomen and internal organs. This visceral fat is biologically active. It changes hormonal signaling, inflammation, liver metabolism, vascular function, and the way muscle tissue responds to insulin.
From there, insulin resistance starts to build. Muscles become less efficient at pulling glucose out of the bloodstream. The liver produces more glucose and more triglyceride-rich particles. The pancreas tries to compensate by releasing more insulin. For a while, the system holds together. It just does so under growing pressure. That is the stage when waist size, triglycerides, blood pressure, and glucose often begin moving in the same direction.
Waist size increases because fat distribution shifts toward a riskier pattern. Triglycerides rise because the liver is dealing with excess incoming fuel. Blood pressure increases because vascular tone, kidney signaling, sympathetic activity, and insulin resistance start to interact in harmful ways. Glucose drifts upward because compensation has limits. These markers travel together because much of the underlying biology is shared.
Why it matters
The term matters because it predicts trouble. Large meta-analyses have shown that metabolic syndrome is associated with roughly a twofold increase in cardiovascular outcomes and a clear increase in all-cause mortality. Its relationship with future type 2 diabetes is even stronger. In other words, this is not just a neat framework for textbooks. It is a real-world warning sign.
It is also common. Population studies in the United States showed a high prevalence years ago, and a 2025 global modelling analysis estimated that about 1.54 billion adults worldwide were living with metabolic syndrome in 2023. This is one of the central patterns of modern chronic disease, not a niche diagnosis.
Why these numbers cluster
A reasonable question is why these specific markers belong together in the first place. The answer is that they often share the same physiological background.
Visceral fat increases the flow of free fatty acids to the liver. The liver responds by producing more triglycerides and worsening lipid balance. At the same time, insulin resistance becomes more pronounced. The pancreas compensates by releasing more insulin to keep glucose under control. That compensation may work for years, but it does not solve the core problem. In parallel, insulin resistance and chronic metabolic overload impair vascular function, raise the likelihood of hypertension, and make further abdominal fat gain more likely. The process becomes self-reinforcing.
That is why metabolic syndrome is best understood as an overlap of interrelated abnormalities rather than a single disease with a single cure. That also explains why a person can have one “acceptable” lab result and still carry substantial cardiometabolic risk.
Criteria for metabolic syndrome
In everyday clinical practice, metabolic syndrome is usually diagnosed when a person has three or more of the following five features:
- increased waist circumference;
- triglycerides ≥150 mg/dL (1.7 mmol/L) or treatment for elevated triglycerides;
- HDL cholesterol <40 mg/dL in men and <50 mg/dL in women, or treatment for low HDL;
- blood pressure ≥130/85 mmHg or antihypertensive treatment;
- fasting glucose ≥100 mg/dL (5.6 mmol/L) or previously diagnosed diabetes / treatment for hyperglycemia.
Waist circumference comes with an important caveat. It is not a single universal cutoff for every population. Thresholds are population-specific. For people of European ancestry, commonly used cutoffs are 94 cm for men and 80 cm for women, but other ethnic groups use different thresholds.
What to do if this assessment suggests metabolic syndrome
The first step is to take it seriously without turning it into a catastrophe. Metabolic syndrome does not mean the system is beyond repair. It does mean that several risk pathways are already active at the same time.
The next step is proper confirmation. Blood pressure should be reassessed rather than judged from a single random reading. Fasting glucose should be checked properly. In many cases HbA1c is useful as well. A full lipid panel matters more than one isolated number. Clinicians also look at body weight, waist circumference, recent weight change, family history, physical activity, sleep, and smoking status. For adults with overweight or obesity, current screening recommendations support active assessment for prediabetes and diabetes and referral to effective preventive interventions when needed.
From there, the real work begins. There is no single “metabolic syndrome pill.” The effective strategy is always combined.
1. Reduce visceral adiposity.
Even modest weight loss can improve the picture. Large diabetes-prevention trials showed that sustained lifestyle change reduced progression to type 2 diabetes, and secondary analyses showed benefits for metabolic syndrome itself.
2. Increase movement without turning it into a heroic project.
A practical baseline target for adults is at least 150 minutes of moderate-intensity aerobic activity per week or the equivalent, plus muscle-strengthening activity on 2 or more days per week. That may sound basic, but this level of consistency has real effects on insulin sensitivity, blood pressure, and weight regulation.
3. Get nutrition into a stable, workable pattern.
That usually means less ultra-processed food, less excess energy intake, more whole foods, more fiber, and a more coherent eating structure. In intervention research, a Mediterranean dietary pattern has been associated with a higher probability of metabolic syndrome reversion in some high-risk adults.
4. Treat the individual components directly.
Persistent hypertension requires its own treatment strategy. Dyslipidemia may require lipid-lowering therapy. Prediabetes and diabetes need their own pathway of follow-up and management. Metabolic syndrome is helpful as a risk frame, but treatment decisions are made using the actual numbers and the person’s broader cardiovascular profile.
5. Check the everyday factors that are easy to underestimate.
Sleep, chronic stress, sedentary time, alcohol, smoking, and vaping all shape cardiometabolic risk more than many people expect. Some people focus only on sugar or only on body weight even though the broader system is under pressure.
The most useful takeaway
The most useful way to think about metabolic syndrome is this: it is not a verdict. It is an early, coordinated warning. Waist size points to risky fat distribution. Triglycerides point to liver overload. Blood pressure points to vascular strain. Glucose points to a compensation system that is working harder than it should.
The earlier that pattern is recognized, the better the chance of changing the trajectory before it becomes type 2 diabetes or a cardiovascular event. That is the real value of the concept. It helps people notice the direction of travel while there is still time to change it.
Sources
- Reaven GM. Banting Lecture 1988: Role of Insulin Resistance in Human Disease. Diabetes. 1988.
- World Health Organization. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. WHO Consultation Report. 1999.
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome. 2005/2006.
- Alberti KGMM, Eckel RH, Grundy SM, et al. Harmonizing the Metabolic Syndrome: A Joint Interim Statement. Circulation. 2009.
- Ford ES, Giles WH, Dietz WH. Prevalence of the Metabolic Syndrome Among US Adults: Findings From the Third NHANES. JAMA. 2002.
- Noubiap JJ, Nansseu JR, Nyaga UF, et al. Worldwide trends in metabolic syndrome from 2000 to 2023: a systematic review and modelling analysis. Nature Communications. 2025.
- Mottillo S, Filion KB, Genest J, et al. The Metabolic Syndrome and Cardiovascular Risk: A Systematic Review and Meta-Analysis. JACC. 2010.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the Incidence of Type 2 Diabetes With Lifestyle Intervention or Metformin. NEJM. 2002.
- Tuomilehto J, Lindström J, Eriksson JG, et al. Prevention of Type 2 Diabetes Mellitus by Changes in Lifestyle Among Subjects With Impaired Glucose Tolerance. NEJM. 2001.
- Ilanne-Parikka P, Eriksson JG, Lindström J, et al. Effect of Lifestyle Intervention on the Occurrence of Metabolic Syndrome and Its Components in the Finnish Diabetes Prevention Study. Diabetes Care. 2008.
- Babio N, Toledo E, Estruch R, et al. Mediterranean Diets and Metabolic Syndrome Status in the PREDIMED Randomized Trial. CMAJ. 2014.
- U.S. Preventive Services Task Force. Prediabetes and Type 2 Diabetes: Screening. 2021.
- World Health Organization. Physical activity guidance for adults.
- American Diabetes Association. Standards of Care in Diabetes—2026, section on prevention or delay of diabetes and associated comorbidities.